
A fit, non-smoking man in his early forties came to see me last year. His cholesterol had always been "fine" on paper — normal LDL, good HDL, no diabetes, blood pressure well controlled. The only thing that worried him was his family history: his father had a heart attack at 48, and an uncle had bypass surgery before 50. Standard risk calculators put him in the "low risk" category. One extra blood test told a very different story.
What Exactly Is Lp(a)?
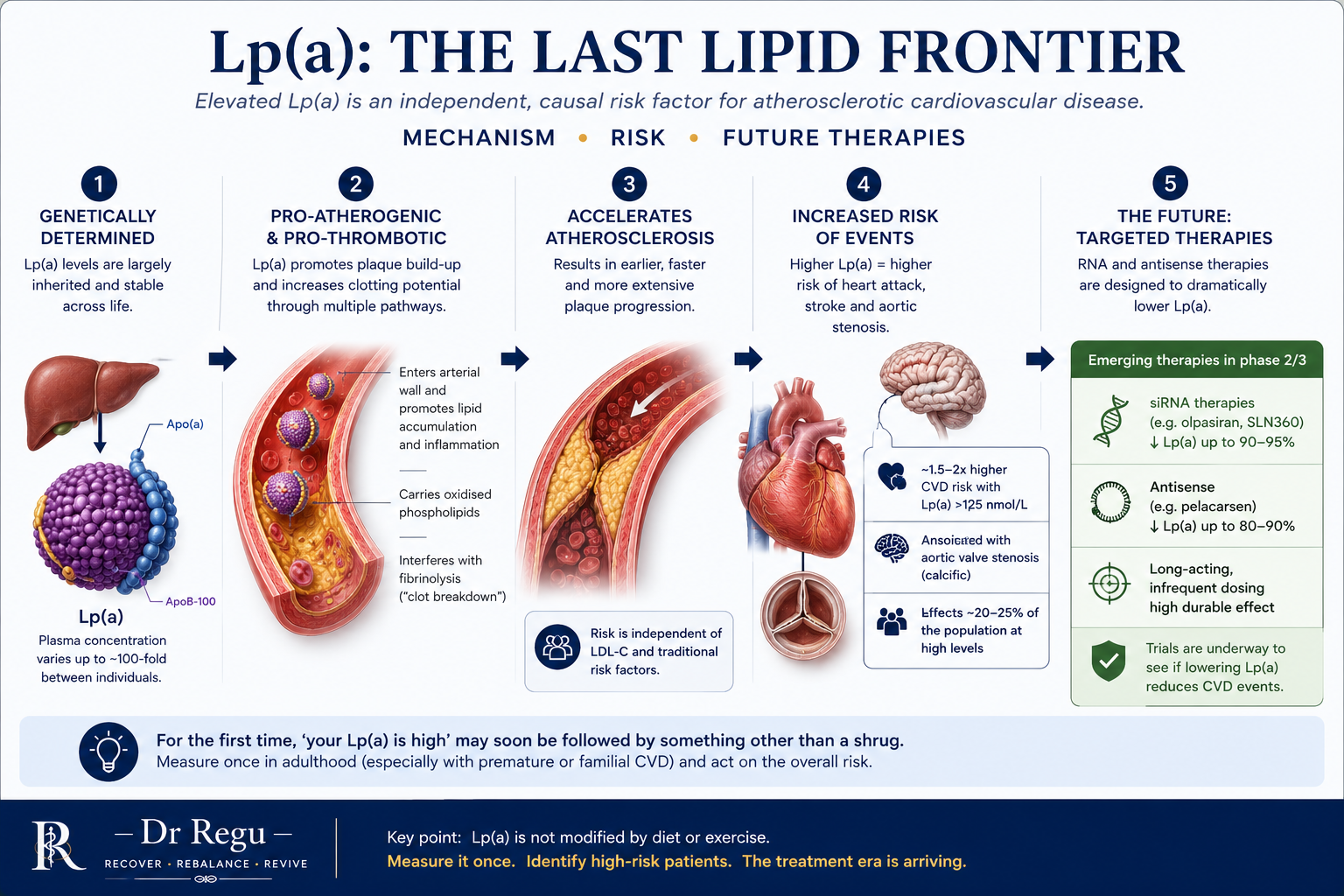
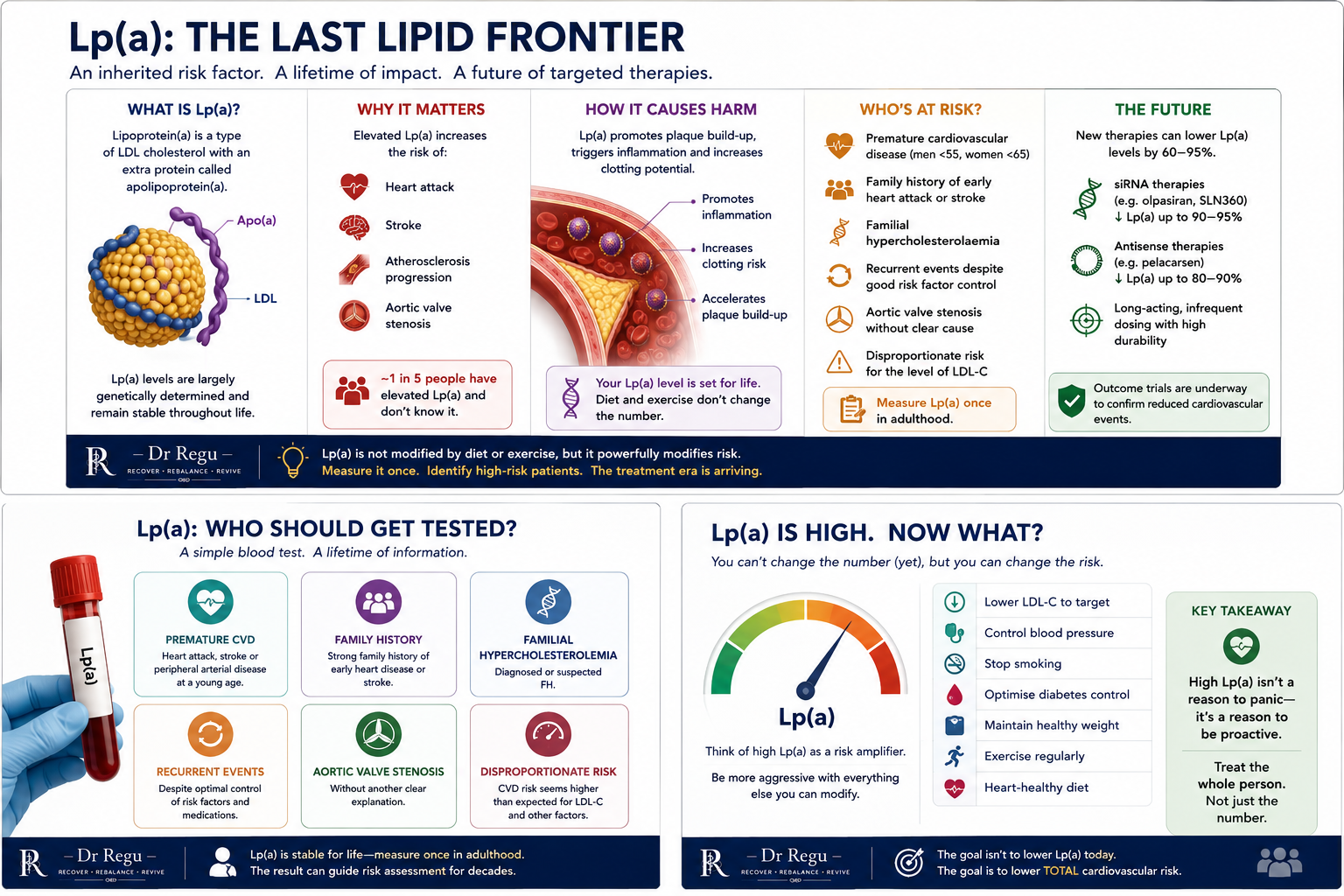
Lipoprotein(a) — Lp(a) — is an LDL-like particle with an extra protein, apolipoprotein(a), attached to it. It is not part of a routine lipid panel, and most people who have had their cholesterol checked have never had it measured. Unlike LDL cholesterol, which responds to diet, exercise and statins, Lp(a) is almost entirely genetically determined. It is set largely by birth and stays relatively stable throughout adult life, regardless of lifestyle.
Lp(a) is both atherogenic (it promotes plaque build-up in arteries, much like LDL) and prothrombotic (it interferes with clot breakdown). That combination makes elevated levels an independent risk factor for heart attack, stroke and aortic valve disease — even when every other cholesterol number looks perfect. Around one in five people carry a clinically elevated level, making it one of the most common inherited cardiovascular risk factors we know of.
Why Has It Suddenly Become Important?
Lp(a) has been recognised as a risk factor for decades, but until recently there was little we could do about it directly — statins barely touch it, and lifestyle change has almost no effect. That is changing fast. A new generation of RNA-targeted therapies — antisense oligonucleotides and small interfering RNA (siRNA) agents including pelacarsen, olpasiran, lepodisiran and zerlasiran — work upstream in the liver to switch off production of apolipoprotein(a) itself.
In early-to-mid stage trials, these agents have lowered Lp(a) levels by anywhere from around 60% to over 90%, sustained for months at a time with infrequent dosing. What we don't yet have is definitive proof that lowering Lp(a) this way reduces actual heart attacks and strokes — the large outcome trials needed to answer that question are underway, with results expected over the next few years. This is the reason Lp(a) has moved from a niche academic interest to a genuine clinical priority: for the first time, a measurable, modifiable target may be within reach.
Who Should Be Tested?
Most major lipid societies now recommend a once-in-a-lifetime Lp(a) measurement for adults, because the level doesn't meaningfully change over time. I'd prioritise testing for anyone with:
- A personal or family history of early heart attack, stroke or coronary disease (men under 55, women under 65).
- A strong family history of cardiovascular disease that seems out of proportion to conventional risk factors.
- Recurrent cardiovascular events despite well-controlled LDL cholesterol and blood pressure.
- Borderline or intermediate calculated cardiovascular risk, where Lp(a) could tip a treatment decision either way.
- A first-degree relative already known to have an elevated Lp(a) — it runs strongly in families, so cascade testing matters.
It's a single blood test, usually not Medicare-rebated outside specific criteria, but inexpensive — and because it only needs to be done once, the cost is a one-off, not an ongoing one.
What Do You Do If It's High?
There is currently no PBS-listed, Lp(a)-specific lowering therapy in routine practice — the agents discussed above are still working through trials. That doesn't mean a high result is something to file away and ignore. In practice, an elevated Lp(a) reclassifies a patient's overall cardiovascular risk upward, which changes how aggressively I manage everything else that is modifiable:
- Treating LDL cholesterol to a lower target than I might otherwise, since the two risks compound.
- Tighter blood pressure control and active management of any insulin resistance or diabetes.
- Smoking cessation and weight management, addressed without delay.
- Referral to a lipid specialist or cardiologist where the result is very high, or the family history is striking.
- Offering testing to first-degree relatives, since a sibling or adult child has a meaningful chance of carrying the same genetic risk.
What This Means for Patients
For patients, the practical takeaway is simple: if heart disease runs in your family — especially if it struck relatively young — ask whether an Lp(a) test has ever been done. It's one blood draw, done once, that can reframe a lifetime of risk assessment and, increasingly, open the door to emerging treatments as they become available.