
A few years ago, most patients had never heard of Ozempic. Today, almost everyone has. Some know it as a diabetes medication. Others know it as a weight-loss injection. Many know it from headlines, social media or celebrity interviews. What often gets lost in the noise is that these medicines may represent one of the most important advances in cardiometabolic medicine we've seen in decades.
The story is no longer simply about losing weight. It's about changing the trajectory of chronic disease.
What Exactly Are GLP-1 Medicines?
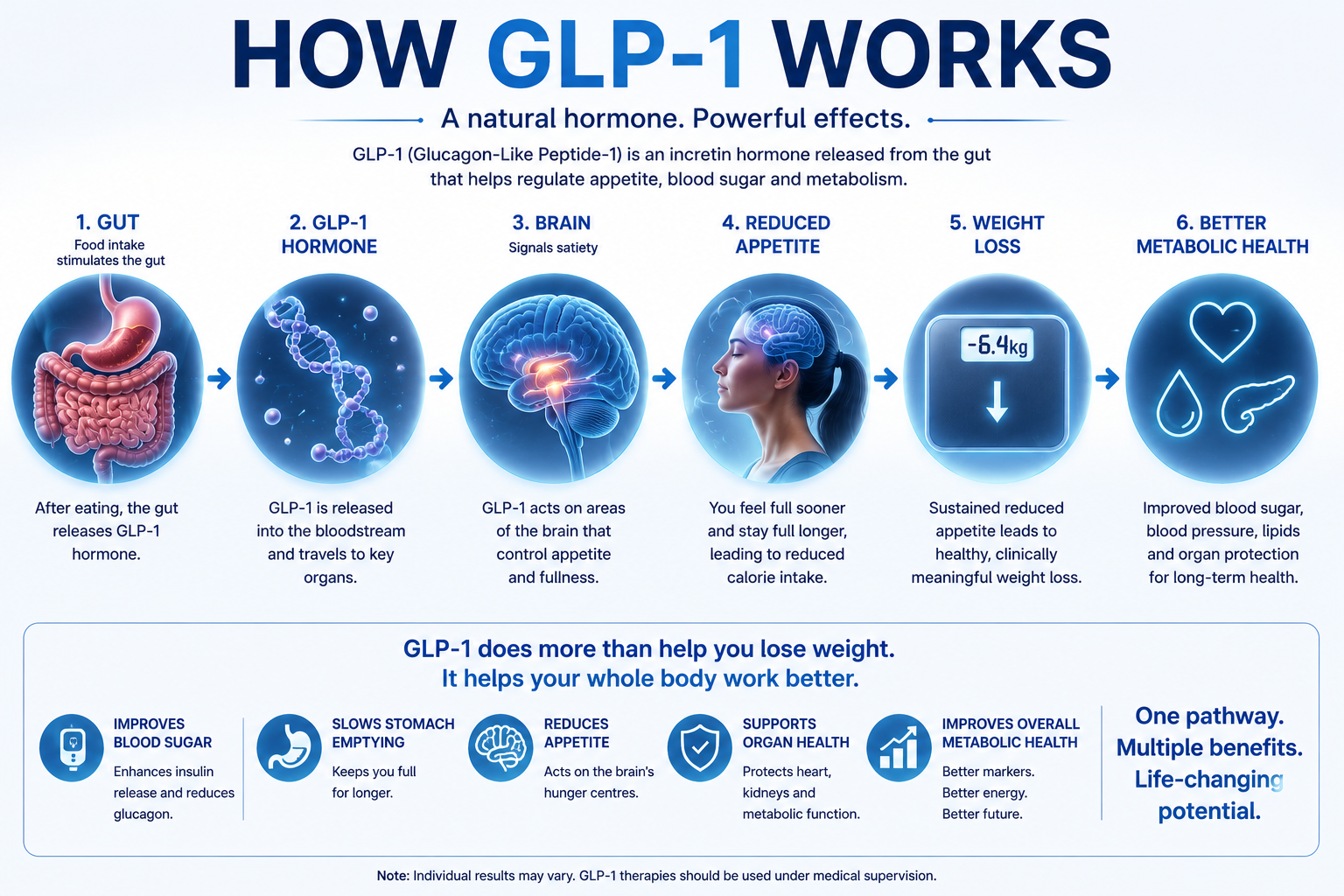
To understand why these drugs have become so important, it helps to understand where they came from. After we eat, the gut releases hormones called incretins. One of the most important is GLP-1 (Glucagon-Like Peptide-1). This hormone helps:
- Increase insulin release.
- Reduce glucagon production.
- Slow stomach emptying.
- Reduce appetite.
- Improve feelings of fullness.
In simple terms, it helps the body manage energy more effectively. Scientists realised that if they could mimic or enhance this hormone, they might improve blood sugar control and reduce weight. They were right.
The Drug That Escaped Endocrinology
Initially, GLP-1 medicines were developed to treat Type 2 diabetes. Then something interesting happened. Patients started losing significant amounts of weight. Not a few kilograms. Sometimes 10%, 15% or even 20% of body weight.
Suddenly endocrinologists weren't the only doctors paying attention. Cardiologists became interested. Nephrologists became interested. Obesity specialists became interested. The public certainly became interested. The drugs had escaped their original purpose.
Beyond Weight Loss
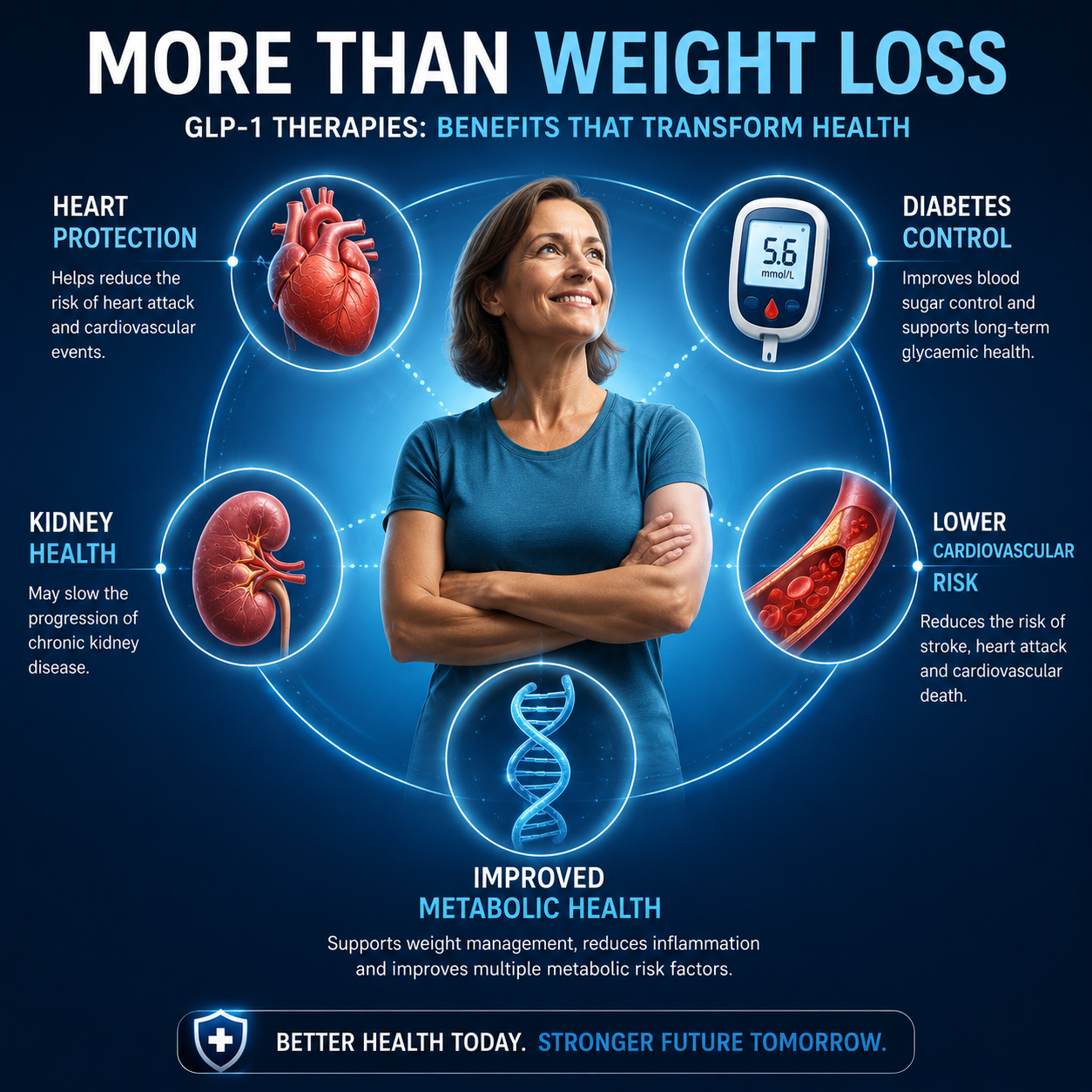
Weight loss remains important. But increasingly, it may not be the biggest story. Large clinical trials have demonstrated benefits extending far beyond the scales.
Cardiovascular Protection
Several studies have shown reductions in major cardiovascular events including heart attack, stroke and cardiovascular death. This is particularly important because obesity and diabetes are fundamentally cardiovascular diseases. Reducing risk matters more than reducing clothing size.
Kidney Protection
Emerging evidence suggests GLP-1 medicines may slow progression of kidney disease in selected patients. Given the growing burden of chronic kidney disease worldwide, this could become increasingly important.
Fatty Liver Disease
Metabolic dysfunction-associated steatotic liver disease (MASLD), previously known as fatty liver disease, is becoming one of the most common liver conditions globally. GLP-1 therapies are showing encouraging results in reducing liver fat and inflammation.
Sleep Apnoea
Weight reduction alone can improve obstructive sleep apnoea, but newer evidence suggests broader metabolic improvements may also contribute.
Whole-Body Health
This is where the conversation changes. Rather than viewing obesity as an isolated problem, we increasingly recognise it as part of a wider metabolic network involving blood pressure, cholesterol, glucose control, kidney function, liver health and cardiovascular risk. Treating one often improves the others.
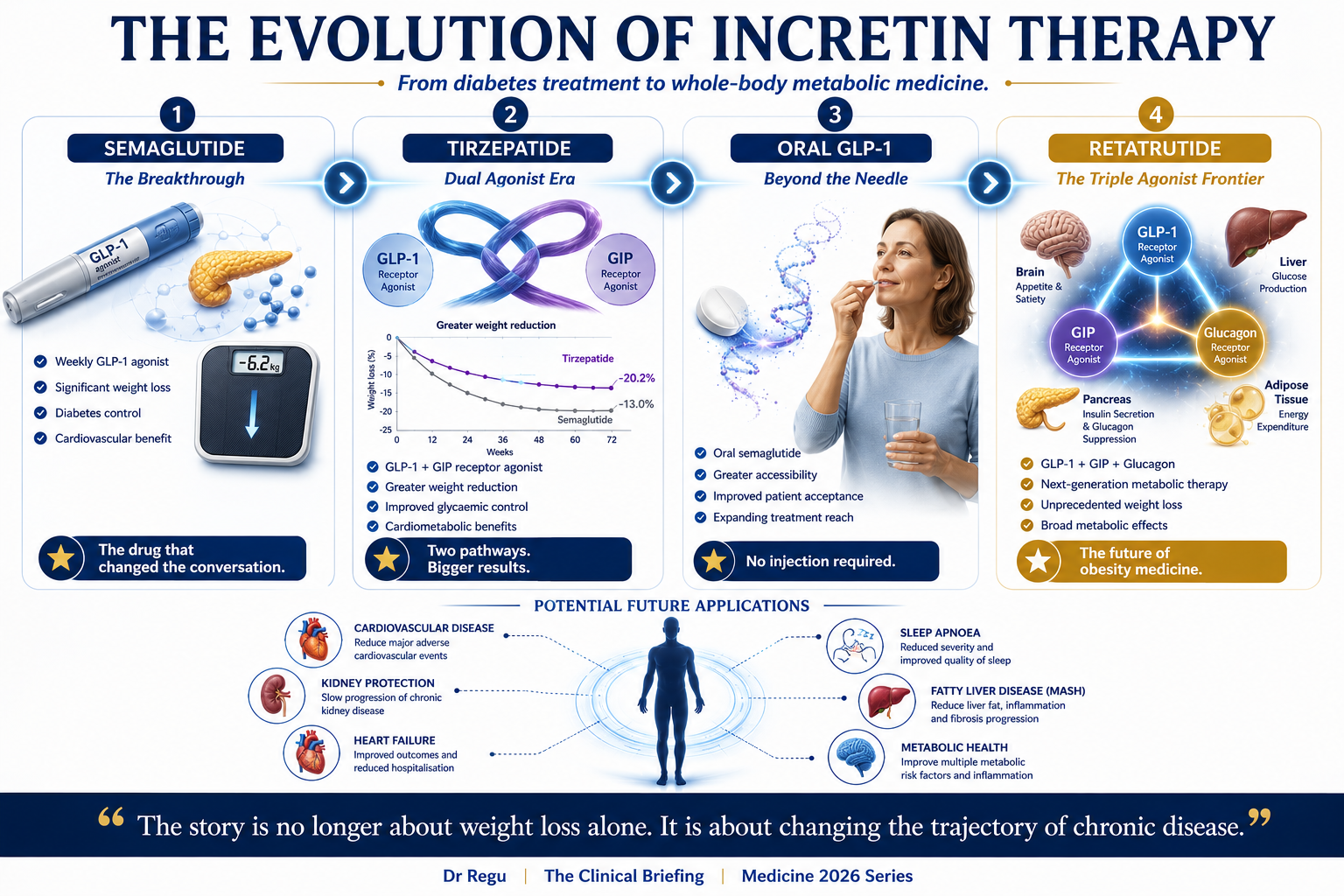
Meet the New Generation
Most people recognise Ozempic. But the field is evolving rapidly.
Semaglutide — the medicine that brought GLP-1 therapy into mainstream awareness. Available under different brand names depending on indication.
Tirzepatide — a dual agonist targeting both GLP-1 and GIP pathways. Clinical trials have demonstrated even greater weight reduction than earlier GLP-1 therapies.
Oral semaglutide — one of the most significant developments may not be a new drug at all. It may be a tablet. Many patients remain reluctant to start injections; effective oral options could dramatically expand access.
Retatrutide — perhaps the most exciting molecule currently under development. A triple agonist targeting GLP-1, GIP and glucagon pathways. Early trial data suggest unprecedented levels of weight loss. The next few years will be fascinating.
The Challenges Nobody Talks About
Whenever a treatment becomes popular, expectations can outrun reality. GLP-1 medicines are powerful. They are not magic.
Side effects — common side effects include nausea, vomiting, reflux, constipation and diarrhoea. Most improve with careful dose escalation.
Cost — access remains a major issue. Many patients who could benefit simply cannot afford long-term therapy.
Supply — demand has occasionally outpaced supply. Balancing access between diabetes and weight management remains an ongoing challenge.
Long-term use — obesity is often a chronic condition. The question isn't simply whether the drugs work. It's whether patients can realistically remain on them long term.
What This Means for Patients
The key message is simple. These medications are not shortcuts. They are tools. Powerful tools. But tools work best when combined with healthy nutrition, physical activity, sleep optimisation, behaviour change and long-term support.
What This Means for General Practice
General practice sits at the centre of this story. We manage obesity, diabetes, hypertension, cardiovascular disease and kidney disease. Increasingly, one class of medication may influence all of them. That doesn't mean every patient should receive a GLP-1 medicine. But it does mean every GP should understand where the evidence is heading.