
For years, CRISPR lived in the same category as flying cars and robot surgeons. Fascinating. Promising. Always just over the horizon. Then something remarkable happened. It stopped being a theory.
Today, patients with previously devastating inherited diseases are being treated with CRISPR-based therapies in the real world. What was once considered impossible is now happening in hospitals. The obvious question is: how close are we to gene editing becoming part of everyday medicine?
What Is CRISPR?
CRISPR is often described as a pair of molecular scissors. That's not a bad analogy. Scientists can use CRISPR systems to identify a specific section of DNA and cut it with extraordinary precision. Once the DNA is cut, cells can:
- Remove faulty genetic material.
- Repair mutations.
- Insert new genetic instructions.
- Switch genes on or off.
In simple terms, CRISPR allows us to edit the genetic code itself. For decades medicine has treated the consequences of disease. CRISPR offers the possibility of correcting some diseases at their source.
Why Is Everyone Talking About It Now?
Because it has finally moved beyond the laboratory. The landmark moment came with Casgevy, the first approved CRISPR-based treatment. Casgevy is used for sickle cell disease and beta-thalassaemia — inherited conditions that have caused lifelong suffering for generations.
Patients often endure repeated hospital admissions, severe symptoms and limited treatment options. For some individuals, CRISPR has delivered something previously unimaginable: the possibility of long-term freedom from disease. That alone makes it one of the most important medical breakthroughs of the decade.
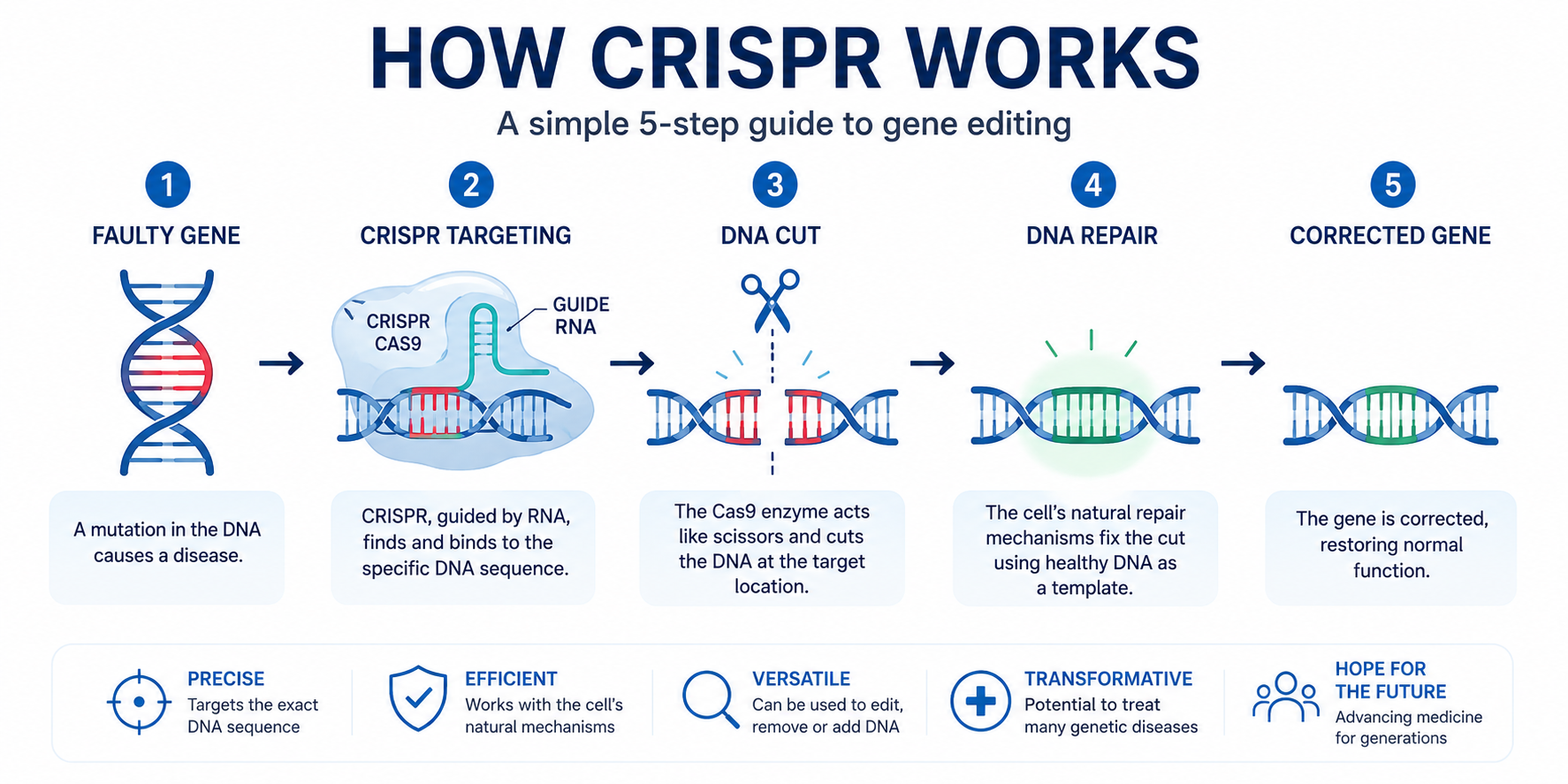
How Does CRISPR Actually Work?
The process is surprisingly elegant. Scientists identify the faulty genetic sequence responsible for disease. A guide molecule then directs the CRISPR system to the exact location. The DNA is cut. The cell's natural repair mechanisms take over. The result is a corrected or modified gene. Conceptually, it looks something like this:
- Identify the faulty gene.
- Target the exact DNA sequence.
- Edit the genetic code.
- Allow the cell to repair itself.
- Restore normal function.
The reality is obviously far more complex, but that is the basic principle.
From Rare Diseases to Personalised Medicine
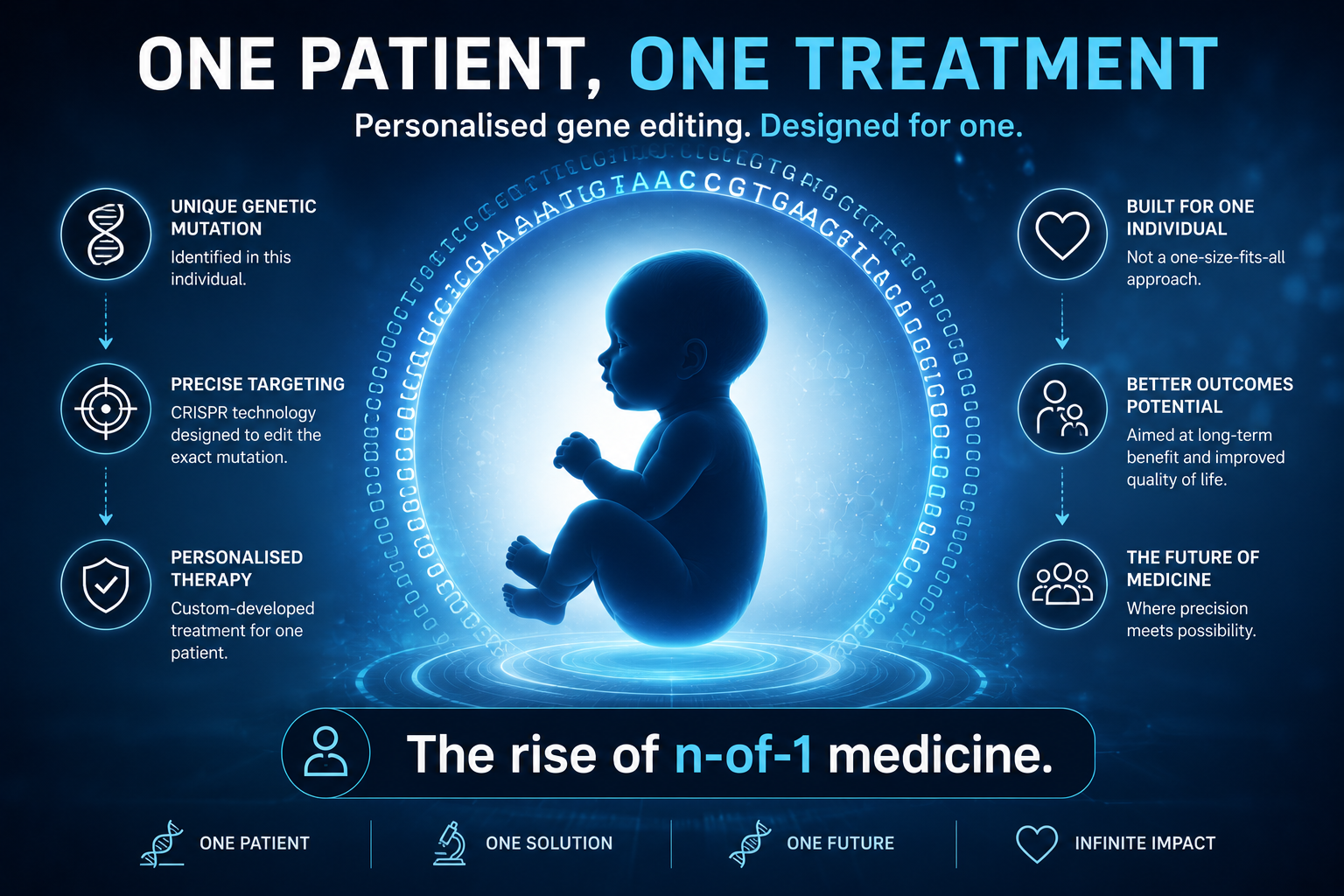
What caught my attention recently wasn't just the approval of CRISPR therapies. It was how rapidly the technology is evolving. In 2025, researchers reported a gene-editing treatment designed specifically for a baby with an exceptionally rare metabolic disorder. Not a treatment for thousands of patients. A treatment for one patient. A genuine "n-of-1" medicine.
The therapy was developed, manufactured and delivered specifically for that child. It represents a glimpse of a future where treatment may be tailored not simply to a disease, but to an individual person's genetic mutation.
Could CRISPR Treat Common Diseases?
This is where things become particularly interesting. Most current CRISPR therapies target rare inherited conditions caused by a single faulty gene — the low-hanging fruit. The bigger prize lies in common diseases. Researchers are already investigating CRISPR approaches for:
- Familial hypercholesterolaemia.
- Cardiovascular disease.
- Liver disease.
- Certain cancers.
- Neurological disorders.
If successful, gene editing could eventually influence conditions that affect millions rather than thousands. We're not there yet. But the direction of travel is clear.
Understanding the Ethical Questions
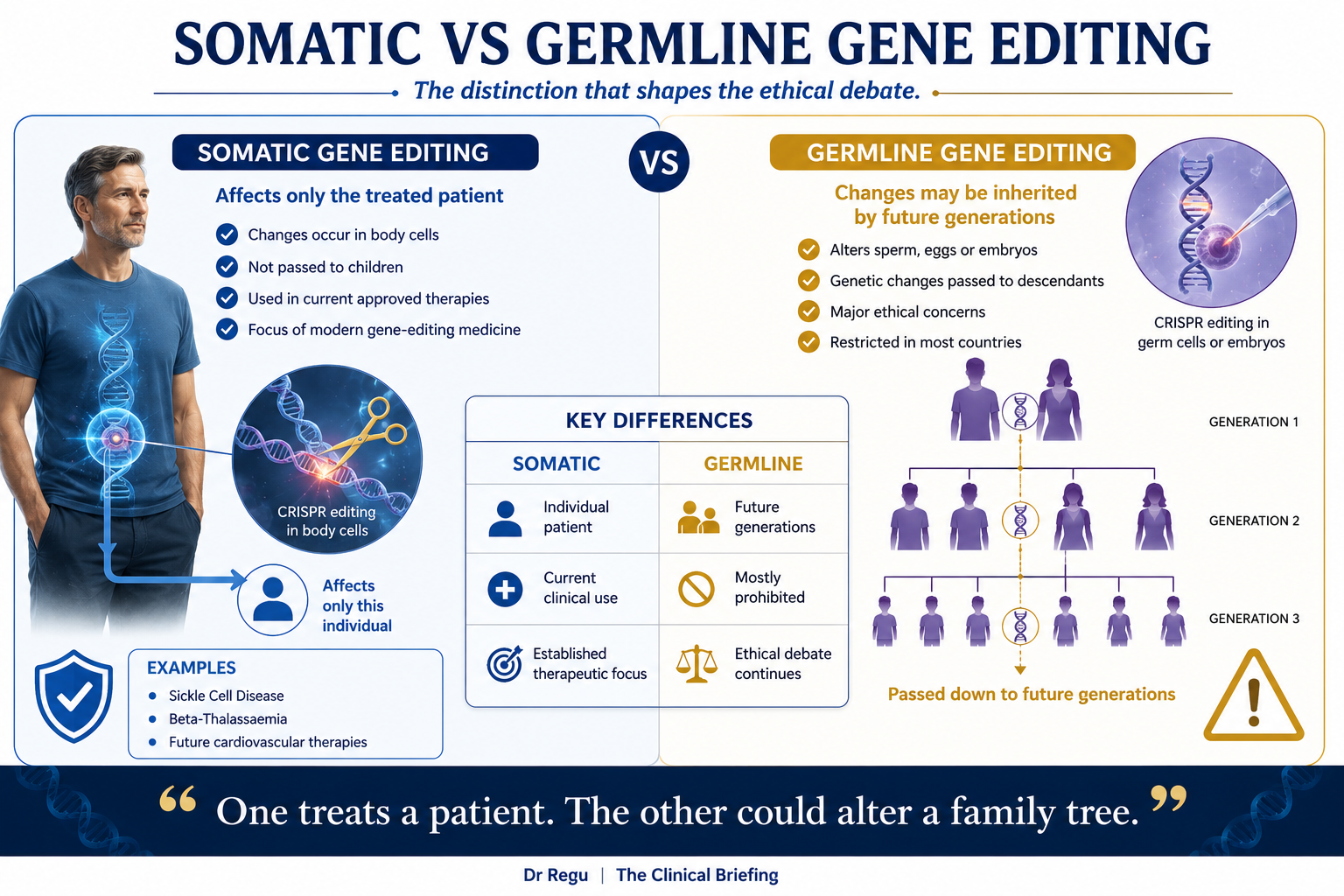
Every major medical breakthrough raises difficult questions. CRISPR is no exception. One of the most important distinctions is between somatic and germline gene editing.
Somatic gene editing — changes are made to cells within an individual patient. The changes affect only that person. They are not passed to future generations. This is the approach currently used in approved therapies.
Germline gene editing — changes occur in sperm, eggs or embryos. Future generations inherit those changes. This remains highly controversial and is heavily restricted in most countries.
Understanding the difference is crucial because many public discussions blur the line between the two. Most current medical applications involve somatic editing, not designer babies.
What Are the Risks?
Despite the excitement, CRISPR is not without challenges. Potential concerns include:
- Off-target effects — the wrong DNA sequence could be altered.
- Long-term uncertainty — some consequences may only emerge years later.
- Cost — current treatments are extraordinarily expensive.
- Access — availability remains limited to specialist centres.
Like many revolutionary technologies, the science has moved faster than affordability.
What This Means for Patients
For most people reading this, CRISPR won't affect tomorrow's GP appointment. But it may affect healthcare sooner than many realise. The first generation of gene-editing therapies is already here. Future generations are likely to become more precise, safer and potentially more accessible. Patients will increasingly encounter headlines about gene editing — understanding what CRISPR can, and cannot, currently do will become important.
The Bigger Picture
Perhaps the most extraordinary thing about CRISPR is what it represents. For centuries, medicine has largely focused on managing disease — lowering blood pressure, reducing cholesterol, controlling symptoms. Gene editing offers something fundamentally different: the possibility of correcting the underlying cause.